On 15 April 2026, OUCRU hosted its first student visit programme, welcoming groups of students from Australian Independent School (AIS) and Sinarmas World Academy (SWA) for a day of discovery, conversation, and hands-on learning.
Designed as part of Public and Community Engagement efforts, the visit aims to open research environment for youth learners by offering a closer look at biomedical research practice in the laboratories, engaging with scientists, and exploring future opportunities in science.
Experiencing Research First-Hand
The visit began with an overview of OUCRU Indonesia by Prof. Kevin Baird, Interim Director of the OUCRU Programme. During the session, students were introduced to OUCRU’s journey as biomedical research unit in conducting clinical trials of diagnostics, drugs, and vaccines for infectious diseases. This session highlighted how OUCRU’s research contributes to improving public health and addressing infectious diseases through collaboration between laboratories, hospitals, and communities.
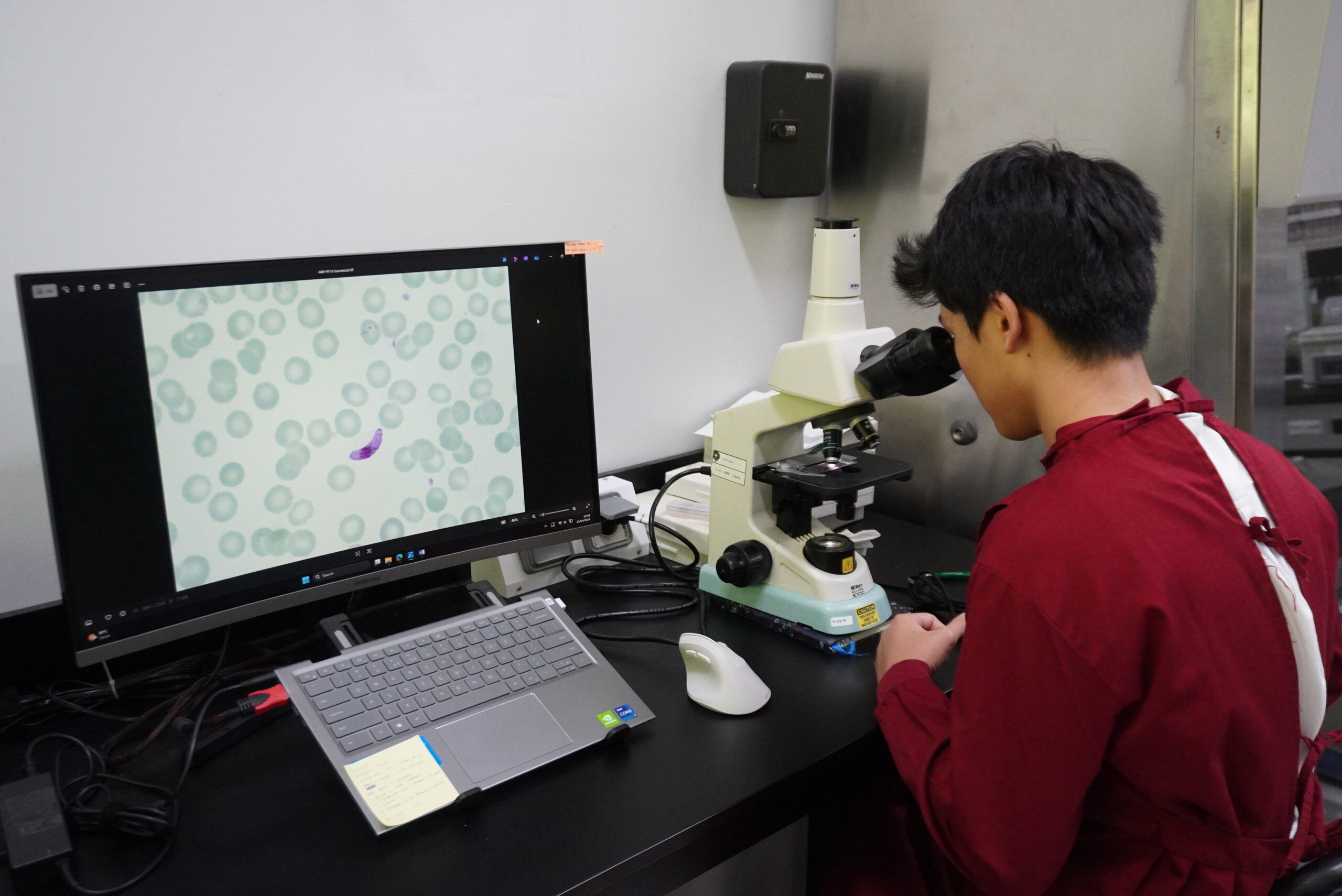
Alongside the OUCRU introduction, students had the opportunity to explore the OUCRU office and laboratories at the Universities of Indonesia & Oxford Clinical Research Laboratory (IOCRL) and Cluster for Infectious Diseases Indonesian Medical Education and Research Institute (IMERI). Students learned hands-on practice of basic laboratory skills in diagnosing infectious diseases, as well as how samples are processed and studied through genomic analysis and sequencing. These experiences helped students see theories they learn in the classroom are applied directly in real-world scientific research.
New Perspectives in Science
As part of their experience, students also participate in a “Careers in Science” panel discussion featuring OUCRU Indonesia research professionals from diverse backgrounds. Covering the world of research, the panel session was moderated by Hanifah Nisrina, Communication and Digital Engagement Officer, and featured Prof. Kevin Baird (Malariologist), Dr Marlous Grijsen (Senior Scientist and Dermatologist), and Suwarti (Infectious Diseases Scientist). Speakers shared their professional journeys into biomedical research and highlighted that there is no single pathway into science. The session also emphasised the importance of youth involvement and the growing need for future talent in biomedical research.
To further encourage interaction with researchers and research support at OUCRU, students participated in an exchange session, “Ask Me About My Job” to explore a wide range of roles behind health research and understand the collaborative nature of scientific work.
Students reflected that experiencing this makes science feel more tangible and achievable. One student shared that the visit revealed “a lot more depth” to research than expected, while another noted that seeing the work firsthand made a career in science feel possible.

“I loved this experience! This is my first visit to a lab and I’m excited to work in research. I think I would want to be like you (science communicator) one day”
– Nayeong, 12th Grade student from AIS
Supporting Future Scientific Talent
As OUCRU’s first student visit programme, this event marked an important step in strengthening engagement between research institutions, educators, and young learners. By opening its laboratories to students, OUCRU aims to nurture curiosity, build scientific understanding, and inspire future careers in research.

“We really appreciate this activity, and we hope to visit OUCRU again with more students.” — Mr. Wei, Teacher at SWA